
I love reading about shoulders and working with them mainly because they’re so complex. It’s not that I really understand it all, but having attended many lectures and a few specific conferences on shoulders, I retain a fascination that probably exceeds that of most personal trainers.
My ‘mentor’ on shoulders is Dr Ben Kibler of Lexington (KY) Sports Medicine Clinic. Dr Kibler got my attention 20+ years ago when he presented at the American College of Sports Medicine annual meeting. Subsequently, I’ve sat in on his presentations and on his ‘clinicals’ there, and attended one or two of his weekend conferences in Lexington just to get a better sense of what the shoulder is about, how it gets injured, what surgeries do and what therapies help.
Allow me to give a brief synopsis of the shoulder joint and how it gets hurt. Then I’ll wrap up with the 8 exercises one will have to do to (1) prevent injury, (2) manage/rehab injury and (3) rehab from surgery. I’ll stop short of the stretches to do as there are too many and each is variable relative to the state of disrepair within the joint.
Anatomy of the shoulder
Dr Kibler speaks of the ball-and-socket joint as more akin to the ball a seal balances on its nose: the seal’s nose is smaller than the diameter of the ball and it has to keep moving to keep it under the ball.
In other words, the socket (glenoid process) of the scapula (shoulder blade) has a smaller diameter than the ball (humeral head of the upper arm bone), somewhat enlarged by the cartilage rim of the socket (glenoid labrum) to cushion the ball and provide a larger base on which to operate.
The socket has to move in synchrony to keep apace with the extremely large ranges of movement of the upper arm, in order to keep the ball in the center of the labrum. This is done by a highly coordinated symphony of muscles around the scapula (periscapular) and around the glenohumeral (scapulohumeral) joint referred to as the scapulothoracic rhythm. That is, the scapula has to move perfectly, and very quickly, on the upper ribs of the back (thorax) to accommodate the movements and positions of the upper arm.
Think about the throwing movement – a classic human behavior dating back to our primate ancestors as they threw rocks or sticks at each other or predators. The arm rises off to the side and over the head, twisting outwardly as it does so – this is the cocking phase; then swoops down vigorously crossing the midline of the chest as it twists internally – the throw and follow through. And all that in less than half a second!
Thus the scapula has to rise, tilt and twist on the cocking phase and descend, twist and tip on the throwing phase. There are finer, more technical terms to describe this pattern but that’s not important. You can always Google ‘throwing mechanics’ to learn more. For now, though, I want you to just get a sense of why the shoulder is so complex and beautiful even in its vulnerabilities.
Pathomechanics of a shoulder injury
The essence of injury, other than impact or collision injuries, is that the rhythm gets broken somewhere along the chain, straining and stressing, or even compressing and ultimately tearing, one or more of the small, fragile structures that hold the ball in the socket: the rotator cuff. Consisting of 4 muscles, generally, these small but very critical muscles pull the ball down and into the center of the socket even as the arm moves and the socket tries to keep up with it. When one or more muscles get pinched between two of the bones or ligaments within the socket region, we call that an impingement. As we age, less blood flow feeds those muscles, so they don’t heal as well as when we were young.
Chronic wear and tear, for throwing or lifting athletes or even office workers, may result in micro-tears that, with one wrong movement, one sudden effort, causes a major tear. Now you have not only pain and inflammation; you also have severe weakness, compromised range of motion and the dreaded ‘frozen shoulder’ (adhesive capsulitis) which is not only a limit on mobility; it’s also more painful, in some cases, than the original tear itself.
What to do to prevent and ‘rehab’ a shoulder injury
If you think about the anatomy and pathomechanics of injury, you will see the rationale for the following exercises right away. But for those who don’t want to delve too deeply into it, here’s the skinny: train the muscles around the scapula that position it to align with the humeral head and train the muscles around the humeral head (the rotator cuff muscles) to keep it centered in the glenoid socket.
First the scapula muscles. As with most rehab exercises, these are usually done with minimal resistance early one, aiming for multiple sets of multiple reps: 3 x 10-30, of each. When pain is gone and tissue is healed, weight can be added so long as the movement patterns are correct!
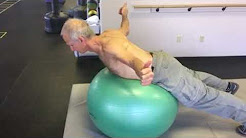
Prone Y
Lying belly down, preferably over a stability ball or weight bench to allow full range of motion, with the arms overhead at an angle and the thumbs turned to the ceiling, raise them up by pulling the lower scapulae together, as in this video:

Prone T
Lying belly down, preferably over a stability ball or weight bench to allow full range of motion, with the arms out to the sides like on a cross and the thumbs turned to the ceiling, raise them up by pulling the lower scapulae together, as in this video:
Prone W
Lying belly down, preferably over a stability ball or weight bench to allow full range of motion, with the arms out to the sides like at an angle with the elbows bent and the thumbs turned to the ceiling, raise them up by pulling the lower scapulae together, as in this video:

Prone I
Lying belly down, preferably over a stability ball or weight bench to allow full range of motion, with the arms down by the sides with the arms externally rotated and the thumbs turned to the ceiling, raise them up by pulling the lower scapulae together, as in this video:

Prone L
Lying belly down, preferably over a stability ball or weight bench to allow full range of motion, with the arms out 90 degrees out to the sides, elbows bent 90 degrees, the thumbs turned toward the ball itself, and the lower arms rotated toward the floor. Then raise them up by pulling the lower scapulae together and rotating the lower arms up toward the ceiling while rotating the thumbs upward, as in this video:

Then for the rotator cuff, the following three exercises will work great.
Upright Open Can
This is done seated or standing. Start with the hands on the front lateral side of the thighs, thumbs turned away from the body. Raise them up to about eye level at a slight angle forward (not directly sideward) as if holding a full, open can of soda:
https://www.youtube.com/watch?v=6AvCBDrJZiM
Tubing External Rotation
With the lowest-resistance tubing attached at the level of your elbow, and your elbow against the ribs (ideally with a towel rolled up between the arm and the ribs) and bent 90 degrees, the forearm flat against the belly, rotate the arm away from the body. Then let it return to the start position sloooowly.


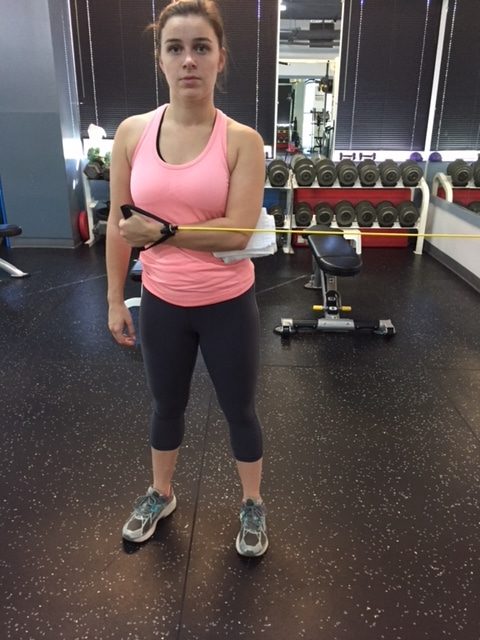
Tubing Internal Rotation
With the lowest-resistance tubing attached at the level of your elbow, and your elbow against the ribs (ideally with a towel rolled up between the arm and the ribs) and bent 90 degrees, the forearm protruding away from the trunk, rotate the arm back toward the body and across the belly. Then let it return to the start position sloooowly. Generally you do fewer sets of these compared to the external rotations.

Conclusion
There are many videos on youtube.com that will demonstrate varieties of these exercises. They will go into excellent detail on body position, alignment, stabilization, etc. that may distract you from the essence of these exercises. Some will make outrageous claims about how doing these/their exercises 2-4 times a week will ensure you don’t have or get shoulder problems, even if you’re a weight lifter. Maybe so, maybe not. But doing the above 8 exercises, 3-4 times a week, which will take all of 15-20 minutes, will help you prevent and rehab most shoulder problems. Of course, you should consult with a doctor or physical therapist to see if any one or more are relevant to your specific conditions, or should not be done at all.
But that said, the first 5 alphabet exercises will work for everyone to enhance proper and better posture. And for those for whom lying belly down on the floor or a ball might be untenable – such as the elderly, those with low back issues that might interfere with positional changes, and the abdominally overweight (discomfort might ensue) – you can practice these standing in front of a mirror, pinching shoulder blades slowly for emphasis.
For the rest of us, think of these as brushing teeth: you can get by without doing so for a while but eventually it’ll catch up to you.







